
EPIDURALS AND CAUDALS
 Many of our patients suffer from pain that relates to disorders in the spinal area, such as disc herniations, previous back surgeries, or complex regional pain syndromes that require nerve blockade in and around the spine.
Many of our patients suffer from pain that relates to disorders in the spinal area, such as disc herniations, previous back surgeries, or complex regional pain syndromes that require nerve blockade in and around the spine.
Since the spinal cord is surrounded by spinal fluid contained in a membrane called the dura, injections done inside the spinal sac are called “sub-dural”, or “spinal injections.” If the injection is done in the space just outside the spinal sac (dura), the injection is called “epi-dural”, meaning “above the dura.” Through the epidural space, injected medicine can reach the spinal sac, the spinal nerves, and can extend both up and down the spine beyond the level of injection. Injection into the epidural space eliminates the need to make a puncture in the dura. This is important to avoid spinal headache.
Epidural injections treat the inflammation, chemical irritation, and other pathology associated with disc rupture and disc bulge causing back and neck pain at the spinal nerve level. Clinical experience shows that many patients have dramatic responses. A recent study demonstrated pain relief for more than 2 years in 78% of 200 consecutive patients.
A retrospective study combining comprehensive rehab with epidural steroid injections yielded a 90% good to excellent outcome with a 92% return to work rate. For patients in both studies, the alternative would have been a major surgical procedure.
Relative to surgery, epidural injections are safe and inexpensive. They are done on an outpatient basis with little or no down time and do not have the morbidity or mortality rates associated with surgery and general anesthesia.
NERVE BLOCKS AND TRANSFORAMINAL INJECTIONS
Selective nerve root block is also known as transforaminal epidural steroid injection. The indications for this procedure are the same for a regular epidural steroid injection with some caveats. This approach to the epidural space is more successful in patients with previous back surgery, or patients that experience radiating pain as opposed to axial pain. It can also be used in a bilateral approach in cases where the medication will need to reach the anterior part of the epidural space. With minimal modification, this procedure can also be used a diagnostic tool.
The patient will be placed in a prone (face down) position, and using live X-ray in an oblique manner; the nerve root exit point (foramen) will be visualized. After numbing the skin over the area, a needle will be directed towards the desired location under fluoroscopic guidance. Before injection the prepared solution the correct position of the needle will be verified using contrast solution.
The procedure lasts about 20-30 minutes. After the completion of the procedure, Band-Aids will be placed at the injection sites, and a nurse will monitor the blood pressure and pulse and will review the discharge instructions with the patient before going home.
RADIO-FREQUENCY LESIONING
 When pain originates from a specific nerve or nerve root, the application of a local anesthetic ( caine drug) can block the pain. This simple test can often predict whether or not long term blockade of that nerve might produce long term pain relief. This applies to conditions where pain originates from a specific structure supplied by a specific nerve.
When pain originates from a specific nerve or nerve root, the application of a local anesthetic ( caine drug) can block the pain. This simple test can often predict whether or not long term blockade of that nerve might produce long term pain relief. This applies to conditions where pain originates from a specific structure supplied by a specific nerve.
Long term nerve block can be done with application of heat, cold, or chemicals. Cryotherapy (cold) is usually very short lived and requires relatively large needle diameters. Chemicals such as phenol or glycerol are often effective but can spread beyond the target nerve to hurt nearby structures. Application of heat energy using radio waves can be an effective way to safely block nerves for long periods of time.
This use of radiofrequency (RF) energy is very similar to cooking with microwaves. The object of RF therapy is not to cook the nerve, but to change nerve transmission without killing the nerve. This is called lesioning the nerve. Permanently injuring the nerve can cause neuropathic ( nerve generated ) pain that can be worse than the original pain.
PERIPHERAL NERVE INJECTIONS
Injection through the nerve root opening (foramen) represents an alternative to injection directly into the epidural space across the lamina or via the caudal canal. This is known both as a transforaminal injection or a selective nerve root block. The injection through the nerve foramen places the needle tip and the medicine into the anterior (front) of the epidural space, close to where the sinuvertebral nerves enter the disc. Since these nerves transmit pain from degenerated discs, injecting near them can often help pain that is resistant to translaminar injection.
On occasion, the interventional pain physician will slip a tiny catheter through the needle into the spinal or epidural space. The catheter can often be directed closer to the source of pain, allowing the medicines to be more effective. Similarly, the catheter can be used to try to break up tiny scars (adhesions) that tug on nerve-sensitive structures. This is called “Adhesiolysis” meaning “breaking apart of adhesions” and is sometimes referred to as the “Racz Procedure.”
In cases where previous surgery inhibits epidural or transforaminal injection, the interventional pain physician may approach the epidural space through the lowest opening to the space, called the “caudal” canal.
Some injections can be done on nerves far away from the spinal area, such as the greater occipital nerve (used to treat some headaches in the back of the head), the lateral femoral cutaneous nerve (used to treat some types of leg pain), or on digital nerves (used to block fingers or toes).
SPINAL CORD STIMULATION
 Spinal Cord Stimulation (SCS) is one method that Interventional Pain Management doctors can use to treat some types of neuropathic (nerve generated) pain. From the beginning it must be emphasized that this technique is an advanced pain management modality that, while effective for certain patients, is not for everyone. All easier and less invasive techniques should have been tried before undergoing a trial of SCS. Only if a trial stimulation is successful will the permanent stimulation device may be implanted.
Spinal Cord Stimulation (SCS) is one method that Interventional Pain Management doctors can use to treat some types of neuropathic (nerve generated) pain. From the beginning it must be emphasized that this technique is an advanced pain management modality that, while effective for certain patients, is not for everyone. All easier and less invasive techniques should have been tried before undergoing a trial of SCS. Only if a trial stimulation is successful will the permanent stimulation device may be implanted.
Spinal Cord Stimulation is usually performed in the operating room under local anesthesia, usually with mild sedation. It consists of placing one or more wires through a needle into the epidural space to stimulate the back of the spinal cord. Each wire has multiple (4-8) electrodes that can be programmed to deliver mild electrical current in various patterns. Under x-ray guidance the wires are maneuvered within the epidural space to produce a vibratory, pain relieving sensation in the area of chronic pain. It takes cooperation and communication between the patient and the physician to accurately cover the entire painful area with the stimulation.
Spinal cord stimulation has been successful in pain management of a subgroup of back pain patients that do not respond to minimally invasive procedures such as epidural injections, and are not candidates for Spinal surgical interventions. This modality has also been successfully used in patients with Failed Back Surgery Syndrome, Neuropathies/Neuralgias, Peripheral Vascular Disease, Arachnoiditis, Phantom Limb Pain, and Complex Regional Pain Syndromes. After initial evaluation, if you are deemed to be a good candidate, educational material in the form of a video tape and brochure will be given to you by your physician. A psychological evaluation might be necessary prior to the procedure; in some situations the insurance companies mandate this evaluation.
DISCOGRAPHY
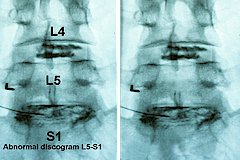 Discography involves placement of a needle inside of a spinal disc for careful, pressure monitored infusion of dye. Since a normal disk is not painful when pressurized to about 80 psi, a disc which produces pain at 60-80 psi might be a source of back and/or leg pain.
Discography involves placement of a needle inside of a spinal disc for careful, pressure monitored infusion of dye. Since a normal disk is not painful when pressurized to about 80 psi, a disc which produces pain at 60-80 psi might be a source of back and/or leg pain.
Provocative discography is a diagnostic tool that is used in patients with mostly axial back pain. If they have a positive response to the procedure, they might be a candidate for surgical fusion, or minimally invasive procedures such as IDET (Please refer to Procedures page).
The discs are soft, cushion-like pads which separate the hard vertebral bones of the spine. A disc may be painful when it bulges, herniates, tears, or degenerates and may cause pain the neck, mid-back, low back and arms, chest wall, abdomen, or legs. Other structures in the spine may also cause similar pain such as the muscles, joints, and nerves. Before performing discography, it has usually been determined that these other structures are not the sole source of pain in a patient (through history and physical examination, review of x-rays, CTs, MRIs and/or diagnostic injection procedures such as facet injections, sacroiliac joint injections, and/or nerve root blocks).
An IV and antibiotic infusion will be started prior to the procedure. The patient will be placed in prone (face down) position and using live X-ray the target disc levels will be identified. This will involve the level(s) that based on the MRI and the patient s symptoms might be responsible for the pain, in addition to an unaffected level as control. After numbing the skin overlying these areas, the needles will be directed inside the discs under fluoroscopic guidance. At this time the physician will inject contrast solution in the disk. This step will not only pressurize the disc space, but it will also show the morphology (shape) of the disc. By asking the patient questions about the quality and location of pain, the physician will determine the pathological disc.
A positive test is experience of pain similar to the usual symptoms the patient experiences on a regular daily basis. The procedure will take 30-45 minutes. Since this a provocative diagnostic test, the patient symptoms might transiently be exacerbated after the procedure. Band-Aids will be placed at the injection sites, and a nurse will monitor the blood pressure and pulse and will review the discharge instructions with the patient before going home.
SPINAL INFUSION AND SPINAL PAIN PUMPS
 One of the advanced techniques for chronic pain or chronic spasticity uses the infusion of medication directly into the spinal sac. Medication is placed into a pump that is implanted under the skin and is infused through a tiny catheter into the spinal sac or epidural space. Like Spinal Cord Stimulation pump therapy is not for everyone or for every type of pain syndrome. Before a spinal infusion device is implanted, all less invasive pain management techniques have been exhausted.
One of the advanced techniques for chronic pain or chronic spasticity uses the infusion of medication directly into the spinal sac. Medication is placed into a pump that is implanted under the skin and is infused through a tiny catheter into the spinal sac or epidural space. Like Spinal Cord Stimulation pump therapy is not for everyone or for every type of pain syndrome. Before a spinal infusion device is implanted, all less invasive pain management techniques have been exhausted.
Spinal infusion involves placing a tiny catheter into the spinal sac or epidural space. These spaces around the spinal sac are separated only by a thin membrane called the dura mater which includes a layer called the arachnoid membrane. Spinal or subarachnoid infusions place medicine inside the spinal sac (inside the dura mater) where the medicine can spread out in the cerebral spinal fluid (CSF) and affect wide areas of pain. Epidural ( above the dura ) medicines flow into the epidural space where the fluid spread is much more restricted by the epidural contents (epidural fat and blood vessels). Where the catheter is placed, and the kind of medicine infused depends on the patient, the type of pain, the duration of infusion, and many other factors.
Rarely does any type of implanted device relieve 100% of pain. However, when chronic pain is unresponsive to any other therapy, partial relief may allow resumption of function. Our goal of 50% pain relief from any invasive therapy often makes the difference between going to work, resuming daily tasks or inactivity. Like all drug therapy for chronic pain, ultimate success is measure by improvement in function.